

TOGA has activated teletrials in ASPiRATION, the ASPiRATION substudies and ALKTERNATE, but has also received ILC2 grant funding to mobilise new clusters for lung cancer clinical trials, to actively implement review of developing clinical trial concepts for amenability to teletrials, as this is a stage of development where design could potentially be modified to better accommodate teletrials, and to raise awareness of teletrials. To assist with clinical trial design that is more amenable to teletrials, TOGA has developed a checklist that is completed for all developing TOGA trials. If possible, the design may be amended to better accommodate teletrials.
The mobilisation of teletrials clusters centres around bringing together lung cancer clinicians/TOGA members of potential clusters, and briefing them of national progress, facilitators and any potential barriers, focusing particularly on facilitating progress through governance requirements. Ideally these establishing clusters would then lobby their particular health service for implementation of the cluster to a point where they can respond to site selection surveys as a teletrials cluster.
TOGA is also coordinating with the other Cancer Cooperative Trials Groups to stay abreast of establishing clusters, liaising with the NHMRC-CTC to adapt existing procedures to accommodate teletrials and seeking progress updates from key leaders of the MRFF-funded activities.
TOGA’s mapping of teletrial clusters
In the first half of 2023 TOGA surveyed its membership in order to establish a preliminary map of existing teletrial clusters as well as provide an overview of potential clusters and those in the process of being established. While the data that we obtained is limited by the participants’ insight and personal views we were able to gain a valuable understanding of the evolving landscape of teletrials in Australia.
Depicted in Figure 1 is the mapping of the respondents’ answers on current teleclusters within Australia. While it was expected that the majority of teletrials are linked to major hospital hubs, it came to our suprise that these were only identified within three states.
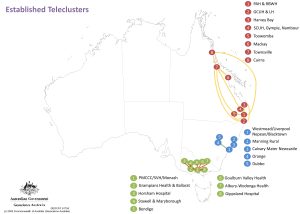
Figure 1: Identification of existing teleclusters
In comparison, our survey results on proposed and developing teleclusters depicted in Figure 2 show promising preliminary findings that this map is shifting to include other states within Australia, as well as uncovering development of clusters that cross state borders.
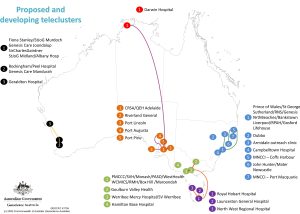
Figure 2: Identification of proposed and developing telecluster
Conclusions based on TOGA’s findings
There are several limitations to keep in mind when interpreting these findings:
- The data is based on a small sample size of 33 responses and is limited to the respondents’ knowledge of telecluster status.
- Clusters limited to hospitals within major cities are not detailed.
However, regardless of the limitations TOGA believes that our research has not only identified the expanding and evolving networks of teleclusters but identified potential sites (such as Hamilton Base hospital in Figure 2) that are not part of teleclusters but could be recruited to expand the network.
If you want to reach out to us in order to help us maintain or update these maps, you can contact us on info@thoraciconcology.org.au
